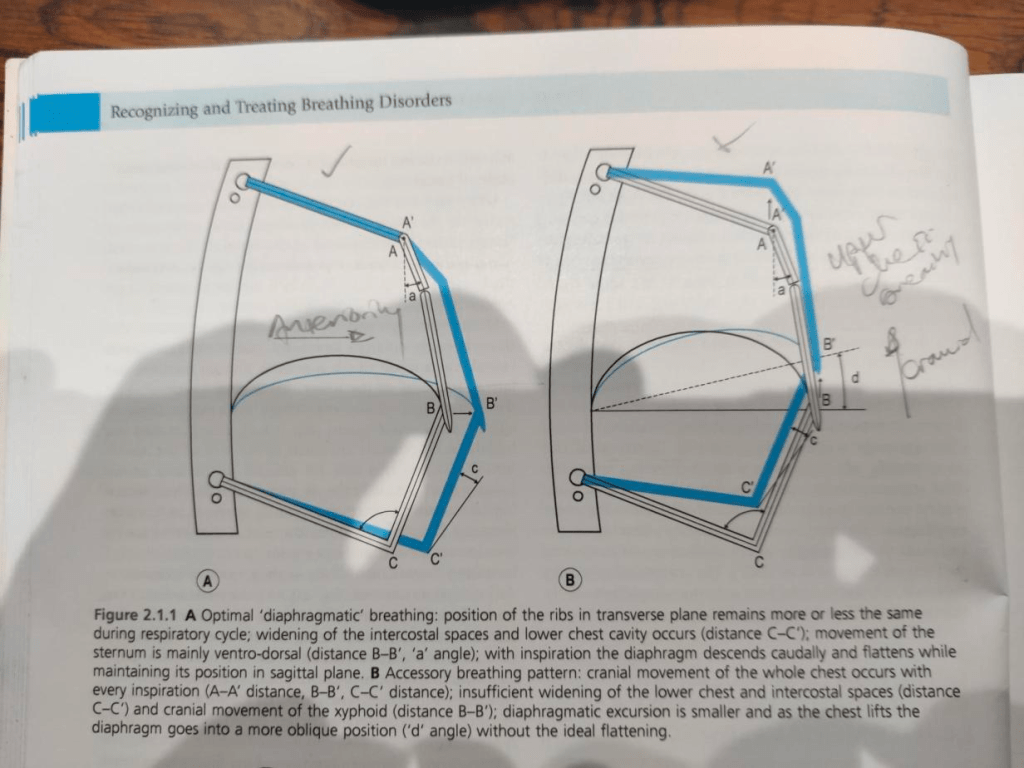
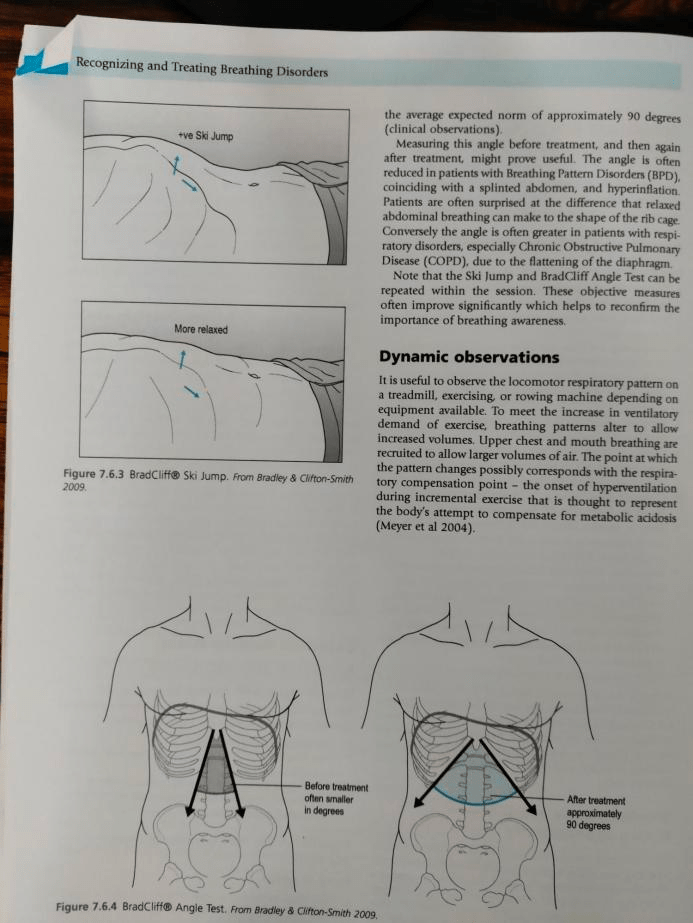
I went down a rabbit hole last week, researching rib flare in runners (or hyper extended ribs) and ended up on a long and interesting journey that took in several books and helped pull together some threads for me, alongside which hopefully has helped developed a deeper understanding around just how key the diaphragm & it’s strength is. Starting from the image I’ve posted above shows optimal diaphragmatic breathing on the left – referencing how the ribcage remains more or less the same. The rights shows a shift, where breathing is more accessory driven, everything begins to lift upwards as opposed to move outwards, with the diaphragm taking on a different shape.
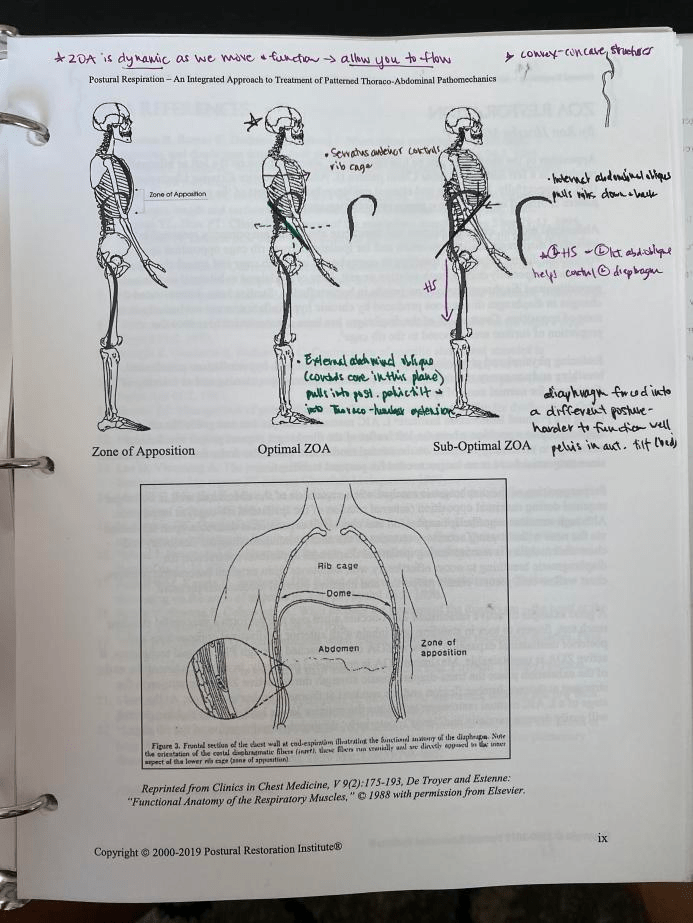
From another angle you can see correct postural / breath alignment on the left and poor alignment on the right. Where this becomes interesting / relevant for rib flare is the direction of the pelvis & ribs on the righthand side, when breathing becomes uncoordinated and the alignment of the diaphragm is oblique, further compromising what it is able to achieve and reinforcing the ribs to flare out.

Looking at this I went to my next book. As I was fairly sure, from what I have learnt that this was going to be centred around the diaphragm being unable to work correctly, due to excessive fatigue I was also curious as to how this related to athletes and why it was presenting at certain points in running.
The first point here is from this page: with the majority of the work of breathing being undertaken by the inspiratory muscles – the diaphragm being key here. The next page begun to add substance to the change in load on the inspiratory muscles as intensity of exercise ramps up

As exercise intensity rises, to cope with this the body has to increase air in / air out. To do this on the amount breathed (tidal volume) is secondary to breath frequency, which rises steeply as exercise intensity reaches its peak. So at high intensities the inspiratory muscles have to hugely ramp up their work, leading to rapid fatigue and drop away in work (as shown in graph b in Fig 1.4)

Reading on Alison McConnell then looks at the impact of this. Showing the “Intolerable zone” as 90-100% of exercise intensity, she postulates that due to this relationship special diaphragmatic/im training needs to be carried out, to make it bearable and effective.
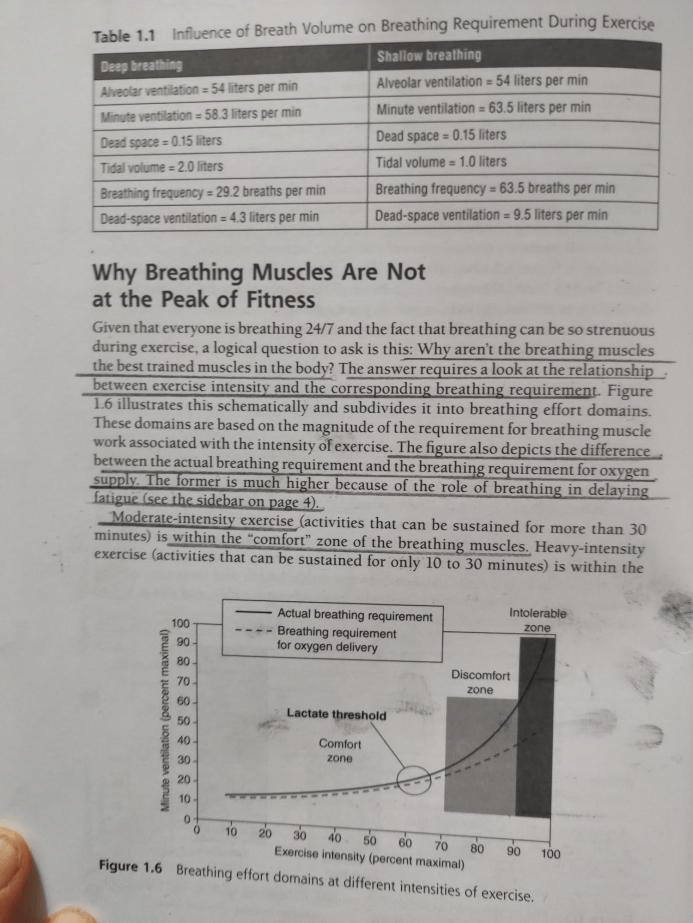
So again how does this relate to Rib Flare – part of the answer to this (I believe) is in the exponentially large shift in load on the inspiratory muscles, that only gets experienced at 90-100% work intensity’s – something that is far less likely to be experienced in the majority of training, but will be in racing situations. If we look at the next page.
McConnell is showing the relationship between the diaphragm and ribs – and as the major inspiratory muscle if this begins to excessively tire and fail in its task then the body will compensate. As stated above and here below – the higher the intensity of work, the greater the need for diaphragmatic work, the more likelihood of fatigue and for some, compensation in rib flare.
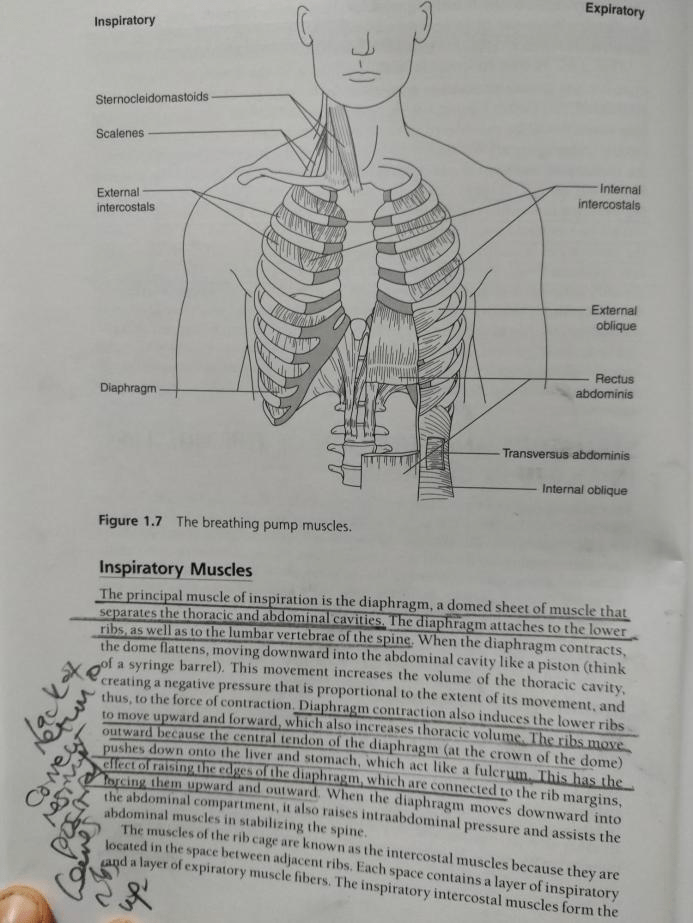
Here McConnell also shows the impact that inflating / emptying a fuller lung has. It takes more energy to inflate something that already has air in it (or at a greater pressure) than if it was empty (at a lower pressure). As exercise intensity rises, lung volume is larger, therefore also increasing the workload on the inspiratory muscles, further creating fatigue.

Carl Stough – given the nickname Dr Breath by the athletes he worked with wrote a really interesting book about his experiences and work, leading up and ending with his time at the USATF 1968 Olympic camp, where he supported the athletes through breathing coordination. Some background on Carl to help draw him into above (and rib flare). He was initially a choir conductor, working with singers on improving their breathing through the use of their diaphragms and focus on the exhale. This then led him to work in VA hospitals with a specific focus on emphysema patients. Here he begun to make connections between improving breathing mechanisms and helping emphysema patients.
He notes here the impact of emphysema on patients
Leading him to build a picture of what poor breathing coordination looked like (oxygen debt leading to a raised chest, pulled upwards by accessory muscles. His work and path then crosses with Coach Giegengack of Yale, where he builds a successful relationship working with Yale athletes, ultimately leading to him being employed by the USATF.
Whilst waiting for this to be finalised he worked with Yale’s swimming team and then moves to Lake Tahoe – it being decided that he wouldn’t instruct the coaches in his method (which he called SIMBIC) but to work directly with the athletes
The narrative that then follows is really instructive with regards his observations on athletes breathing & what he begins to see as extended ribs (or hyper inflated), drawing parallels for him with the emphysema patients he dealt with. Here, bottom right you can see he notes how surprised he was at the poor breathing mechanics of highly trained athletes, this being magnified due to the altitude of Tahoe and the increase in oxygen debt from training there.

He begins to discuss the work of the diaphragm, on the right hand page below and what happens when it is weakened (or not developed in coordination with other breathing muscles.
Continuing here he makes the key observations:
It is here that he states the key element to resolve is the exhale (as he experienced when working with emphysema patients) and how he began to work on this with the athletes that came to see him. What is great above is that he explains how he showed athletes photos of emphysema patients – pre and post treatment to help support the work he wanted to do with the athletes. Bringing this back to rib flare and the athlete, Stough then explains why Tahoe was such a great environment for him to work in:
And in this chapter he comments on what he saw as a key finding in the athletes:

The bottom point something worth exploring, the over development of chest muscles creating an imbalance in the breathing mechanism and resultant issues. Having re skimmed the book – trying to find the most relevant parts, it seems Stough saw the exhale & breathing coordination as key, with a focus on integrating correct and full use of the diaphragm throughout to help remove the issues athletes presented, which mirrored emphysema patients – resulting in an inability to clear the lungs of air properly, which led to compensatory issues.
SO – with this in mind, what can be done, how did Stough deal with it and is there anything else that we can do to help. Stough is never particularly specific about his technique in his book, hiding it behind each athlete having a protocol that worked for them. The closest I could find was getting athletes to take a long, low (deep) breath in then exhale as slowly as possible by repeatedly counting (whispering) from 1-10 until they could count no more. Vocalising will push all the air out of the lungs. I can’t find the page again now, but do remember him writing that with some athletes he would combine this by applying gentle downward pressure onto their lower ribs, re familiarising the body (and nervous system) with the joint movement of an ascending diaphragm and descending lower ribs. This technique is something I’ve had athletes do if they are getting worried about shortness of breath / tightness in the chest as they run, and a good start in re-training the breathing mechanism.
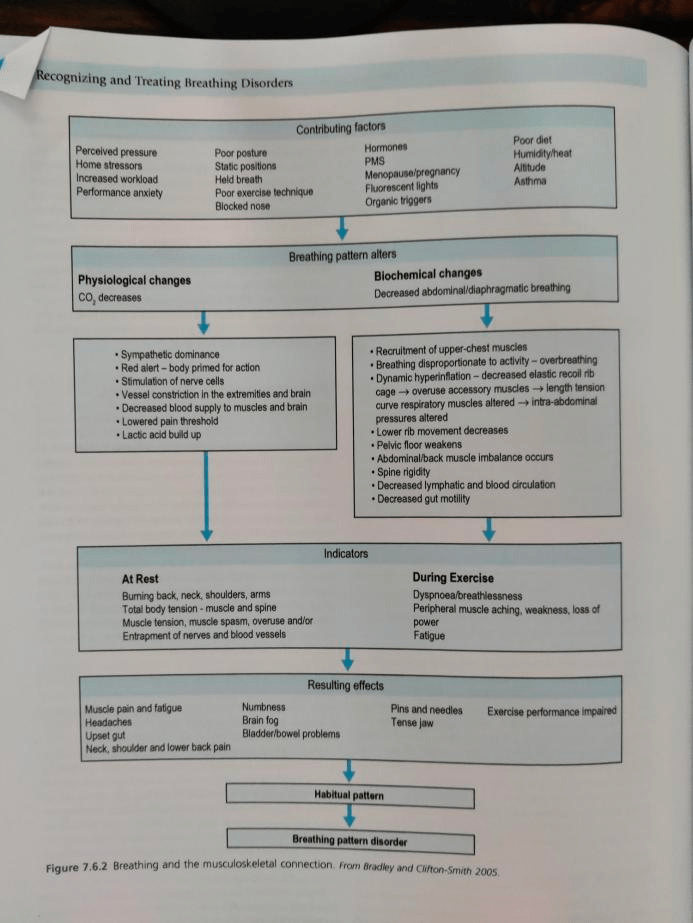
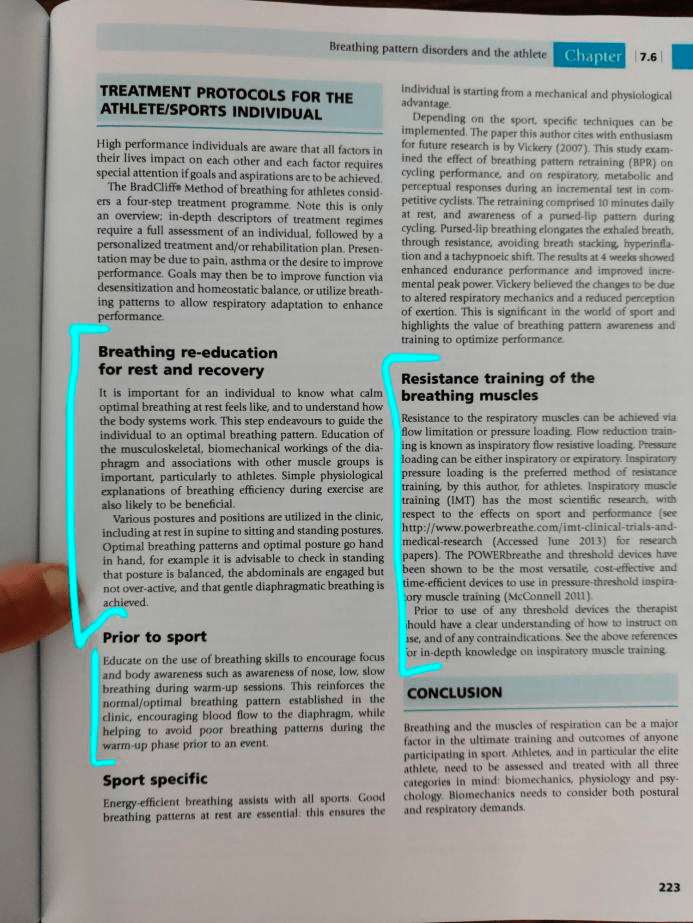
But there must be more – and with the history and experience of Stough behind me I went back to Leon Chaitow’s book, McConnell’s book and Belisa Vranich’s book to look for assessing and other remedial methods and discovered more to layer on Stough’s work in 1968. This book is excellent and I’d advise all to check it out. In Chapter 7.6, written by Tania Clifton-Smith is entitled Breathing Pattern disorders and the athlete.
Some key takeaways from this chapter is a great table on how breathing pattern disorders (BPD) can arise – and here this relevant to hyper inflated ribs, as this a BPD:
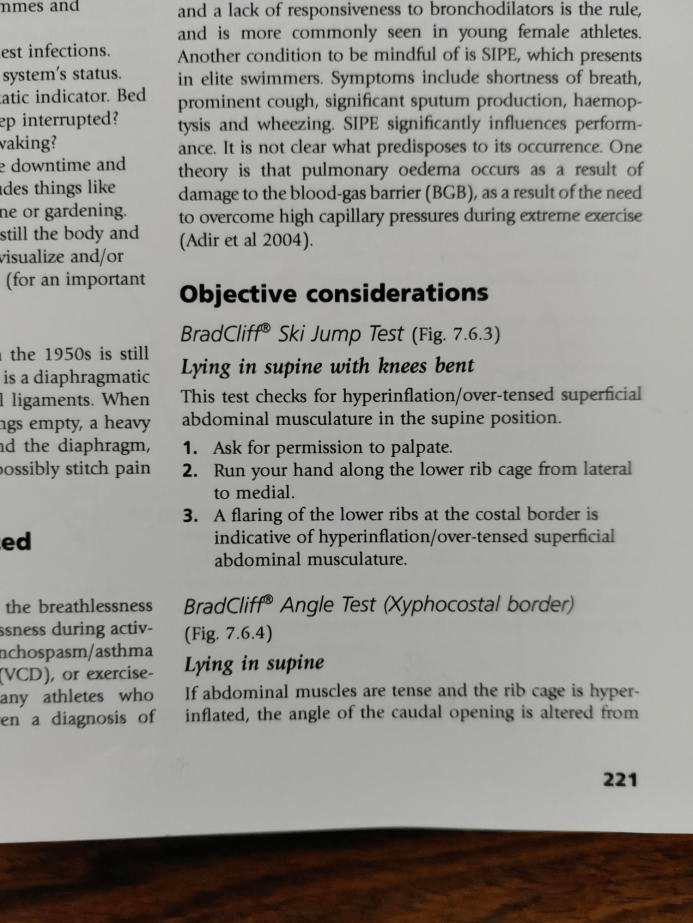
She offers a test that you can do for hyper inflated ribs:
And finishes with an overview on breath retraining.
On the second page she references back to Alison McConnell – who I was using at the beginning of this – for breath retraining. I’ve not used McConnell’s trainer as: 1. I’m more inclined to work without such extreme resistance, to get an athlete to focus on the somatic sensations (as Stough did) around breathing co-ordination, but that’s not to say her methods aren’t really sound.
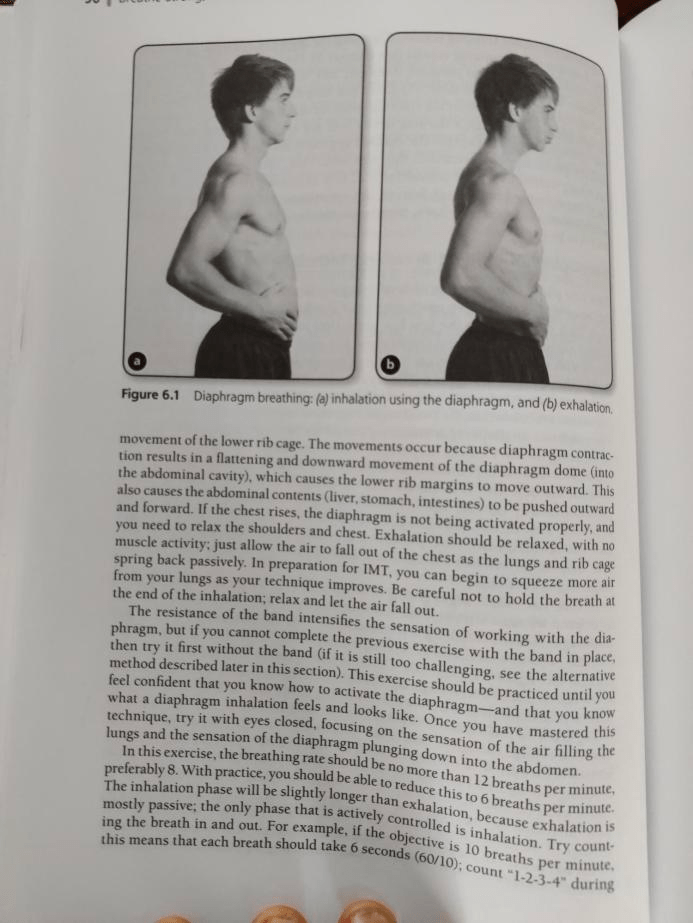
Where I do like McConnell’s work is on developing an efficient breathing technique for an athlete and once again reconnecting with how you should breathe. The next 3 pages are her method for reintroducing good breathing patterns:

Lastly there is another assessment I found – which I find really helpful, especially as for most athletes hyper inflated ribs may only appear under pretty extreme circumstances, but at absolutely key moments (thinking back to earlier when McConnell explains why this is & Stough sees altitude as magnifying more taxing conditions) which is pretty instructive in how well coordinated breathing is AND MORE IMPORTANTLY, how able it is to cope with the increased load of increased intensity.
Belisa Vranich talks about Location of movement (which direction does your body move in when you breathe) and Range of motion (the difference between inhale and exhale. She has a simple assessment to measure this, which put together is your Breathing IQ
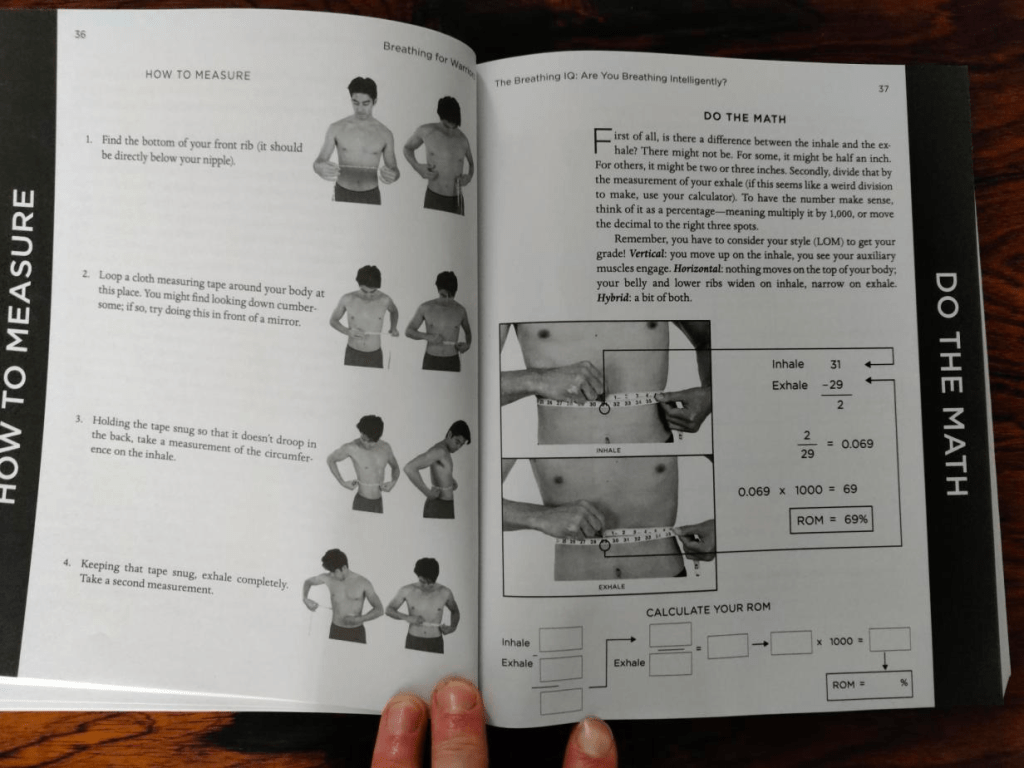

This giving a really good guide on how much you actually exhale versus your inhale. So that’s my journey into rib flare – hopefully helpful and useful.
To summarise it would seem to be unlikely to present until at a high work load and it’s not unusual for top class athletes to have disordered breathing of some nature, that shouldn’t be assumed absent due to their level of ability. It seems a result of dysfunctional breathing, centred around the diaphragm being unable to do it’s work correctly and the body compensating.
The diaphragm being unable to work properly leads to stale air being left in the lungs and the rib cage being forcibly pulled upward on the exhale to try and empty / refill.
Assessments at rest can centre around either the BradCliff Ski jump test or a breathing IQ assessment. Moving forwards retraining the diaphragm is the first course of action – correcting the breathing patterns and then strengthening the diaphragm under resistance.
For more detailed and advanced methods of doing this Alison McConnell’s book.
Pavel Tsatouline (of Strong First) has a good technique that is mentioned in Belisa Vranich’s book. “Lie down on the ground, put a straw in your mouth, pinch off your nose, and just breathe. When you can comfortably do that line up two straws to make it longer, Then go to three straws, which is usually enough” Breathing under resistance seems key – and connecting with the process
I then had some wonderfully helpful feedback from another coach, adding material from PRI to my knowledge base: